We have 3 Action Item today at Issue 2 (1) and 3 (2)
Summary of Issues
At Issue 1. we see LAWMAKER BLASTS PLAN TO CAP MILITARY PAY RAISE. Proposal to cap pay for 4th straight year meets opposition.The Personnel Subcommittee chair speaks out against a proposal to widen the military pay gap. (See Issue 1 below for the details. GF)
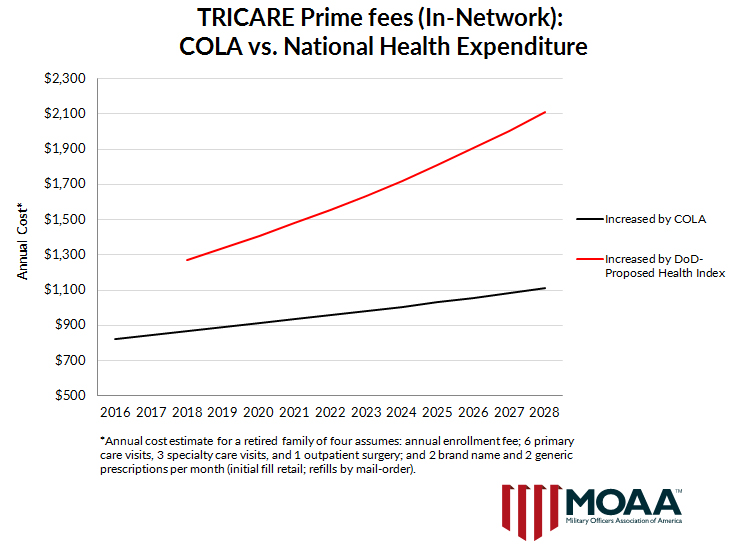
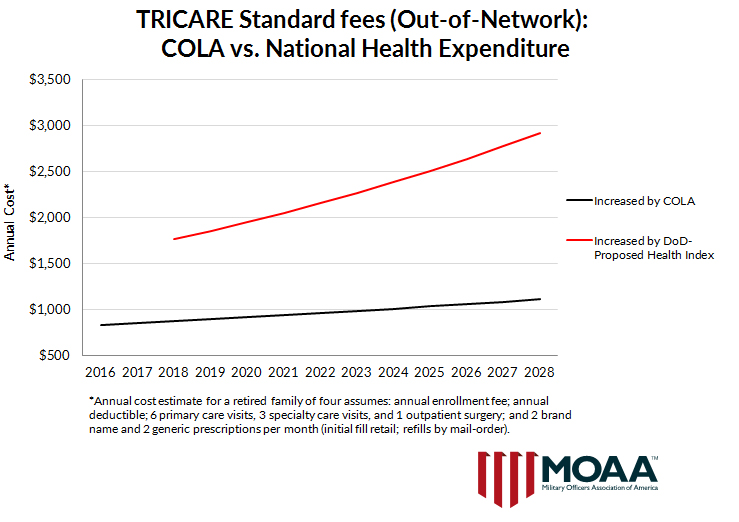
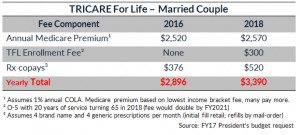
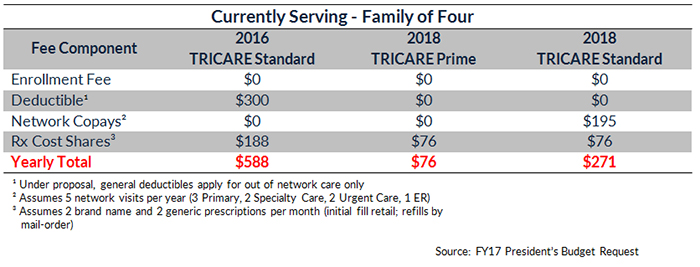
At Issue 2. we see YOU STILL HAVE TIME TO ACT The military deserves top-tier health coverage. Urge Congress not to break faith with those who have served. (Click on YOU STILL HAVE TIME TO ACT here or above to take you the Legislative Action Center screen where you can scroll down and edit the draft message if desired and verify or enter your personal information before hitting the Send Message button to send messages to your three Legislators. GF)
At Issue 3. we see ELIMINATING THE WIDOWS’ TAX. Military survivors deserve better. Urge your legislators to fix this unfair situation. (See Issue 3 below for the details and to send two messages to your Legislators. GF)
At Issue 4. we see SUBMIT YOUR RESOLUTION. Help shape MOAA’s future. Any MOAA member may propose a resolution addressing a legislative or policy issue related to MOAA’s missions and goals. (If you are MOAA member and are interested, click on SUBMIT YOUR RESOLUTION here or above to submit a propose a resolution. GF)
Collectively We Can and Are Making a Difference
FOR ALL, Please feel free to pass these Weekly Legislative Updates on to your group of Veteran Friends –
don’t be concerned with possible duplications – if your friends are as concerned as we are with Veteran issues, they probably won’t mind getting this from two or more friendly sources
ISSUES
Issue 1. LAWMAKER BLASTS PLAN TO CAP MILITARY PAY RAISE
March 11, 2016
At a Senate Armed Services Committee hearing Tuesday, Personnel Subcommittee chair Lindsey Graham (R-S.C.) told service chiefs he’s not happy DoD is proposing yet another reduced military pay raise for 2017.“For the last three years, this administration has failed to allow servicemembers’ pay to keep up with the private sector wage growth,” said Graham. “This is the fourth year in a row where the department is shortchanging servicemembers.”
The proposed 1.6 percent pay raise is being touted by DoD as the largest raise in the last four years. However, it is still below the average American’s 2.1 percent raise, as measured by the Employment Cost Index (ECI). If Congress doesn’t reject the Pentagon proposal, the cumulative four-year pay gap will increase to 3.1 percent.
Graham also took issue with the Pentagon’s proposal to make changes to the new blended retirement system scheduled to take effect on Jan. 1, 2018 for new entrants.
Under current law, the new system cuts military retired pay by 20 percent, but provides up to a 5 percent government match to servicemembers’ deposits in federal Thrift Savings Plan (TSP) accounts. Government matching begins when a servicemember reaches three years of service. DoD’s budget proposes delaying government matching until the fifth year of service.
This proposal directly counters one of the main reasons why Congress originally approved the change to retirement: to provide a retirement benefit to more servicemembers, especially the majority who do not stay for twenty years.
“Let me be clear. It is our commitment to the many servicemembers who go out on deployment before reaching their fifth year of service that they, too, have earned some retirement,” said Graham.
MOAA agrees with Sen. Graham’s concern on both the pay raise and TSP matching issues
Issue 3. ELIMINATING THE WIDOWS’ TAX
March 11, 2016
Survivors of deceased servicemembers are required to forfeit all or part of their military Survivor Benefit Plan (SBP) annuity when military service results in the death of their sponsor. This is often referred to as the ”widows’ tax.”
Retiring servicemembers may purchase SBP insurance coverage to provide their surviving spouse up to 55 percent of their retired pay in the event of their death for any reason. SBP coverage is automatically provided for deaths that occur on active duty.
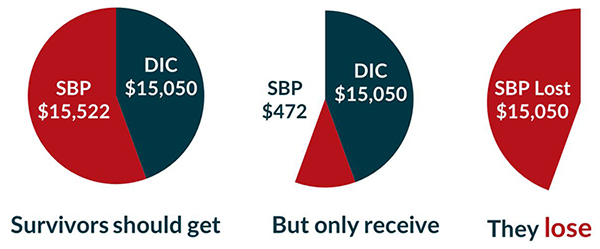
If death is determined by the VA to be service-connected, the VA pays the survivor an additional payment called Dependency and Indemnity Compensation (DIC). Currently DIC recipients receive $1,254 monthly, or about $15,000 a year.
However, under the current law, the amount of DIC awarded must be deducted from military SBP annuities. The widow’s tax wipes out most – if not all – of the SBP for the vast majority of survivors.
For instance, in the case of an E-6:
In multiple Congresses, lawmakers acknowledged the inequity and co-sponsored corrective legislation to recognize SBP and DIC are paid for different reasons. SBP is a servicemember-purchased annuity, whereas DIC is an indemnity payment when military service caused the member’s death.
Further, service-disabled retirees have limited opportunities to purchase additional life insurance, and policies that are available impose exorbitant premiums.
No other federal surviving spouse is required to forfeit his or her federal annuity because military service caused his or her sponsor’s death. Additionally, the offset does not apply to surviving military children – only to the spouse.
Tasked by Congress to review the widows’ tax in October 2007, the Veterans Disability Benefits Commission (VDBC) agreed with MOAA and other veterans associations that when military service causes the member’s death the VA indemnity compensation should be paid in addition to the SBP annuity, not subtracted from it.
In 2008, Congress authorized a Special Survivor Indemnity Allowance (SSIA) as partial recompense for the SBP-DIC inequity. Then-House Armed Services Committee Chairman, Rep. Ike Skelton (D-Mo.), expressed the intent to continue increasing the SSIA and ultimately phase out the widow’s tax. SSIA is $275 per month in FY16, and will rise to $310 per month in FY17, covering about 25 percent of the SBP-DIC offset.
However, the legal authority to pay SSIA expires on Oct 1, 2017. Unless Congress repeals the SBP-DIC offset or extends the SSIA authority this year, SBP-DIC survivors will suffer the additional loss of the SSIA, totaling $3,700 annually.
MOAA believes the SBP-DIC offset should be repealed. Because of the current budget environment, securing sufficient funding for a total repeal – approximately $6.5 billion – will be difficult. If full and immediate repeal is not feasible, SSIA should be extended and increased to continue the path toward phasing out the offset.
There are two current bills that would repeal the widows’ tax. Click the links to send your legislators messages supporting H.R. 1594 sponsored by Rep. Joe Wilson (R-S.C.) and S. 979 sponsored Sen. Bill Nelson (D-Fla.).
(Click on H.R. 1594 here or above to send a message to your Representative. After clicking on the Bill number, at the next screen, the Legislative Action Center, scroll down and enter your Zip Code at the lower right of the screen and hit Go to get you Take Action and Compose Message section. There the message can be edited if desired. Then check or enter your personal information before hitting Send. Then come back and repeat the process by clicking on S. 979 here or above to send a message to your Senators. GF)
That’s it for today- Thanks for your help over the years!